
Here is the unfashionable take: the FDA’s enforcement wave this spring did not expose a crisis of bad actors. It exposed a crisis of bad questions. Everyone is suddenly asking “is this vendor licensed,” which is the right question asked a year too late and, on its own, still an incomplete one. The question nobody wants to sit with is whether the compound itself has earned the confidence people are placing in it, licensed seller or not.
I’ve spent the year reading the same threads, the same DMs, the same “which site do you trust” posts, and I think the industry, and frankly a lot of the coverage of it, has settled on a comforting story: gray-market bad, licensed-clinician good, problem solved. That story is about 70% true. The other 30% is where people are going to get hurt next, precisely because they think the crackdown fixed something it only partially touched.
What actually happened, and why it’s being misread
On March 3, the FDA told 30 telehealth companies to stop marketing compounded GLP-1 products with false or misleading claims, including implying the compounded versions were equivalent to approved drugs [8]. Commissioner Marty Makary put it bluntly: compounders “should not try to circumvent FDA’s approval process by mass-marketing compounded drugs” [8]. Three and a half weeks later, on March 31, the agency went after research-peptide sellers, Gram Peptides among them, and said flatly that a “research use only” sticker does not exempt a product from human-use scrutiny [9].
That is a real, meaningful correction. It is not, however, a verdict on the compounds themselves. The enforcement actions are about marketing and labeling, about who is allowed to say what to whom. They tell you almost nothing new about whether BPC-157 works, or whether retatrutide is safe long-term, or whether the peptide in your cart has decades of human trial data behind it or basically none. That distinction, evidence versus oversight, is the one I keep watching people collapse into a single “trustworthy or not” binary. It isn’t one axis. It’s two.
The case for treating oversight and evidence as separate scores
Run the numbers side by side and the split becomes obvious.
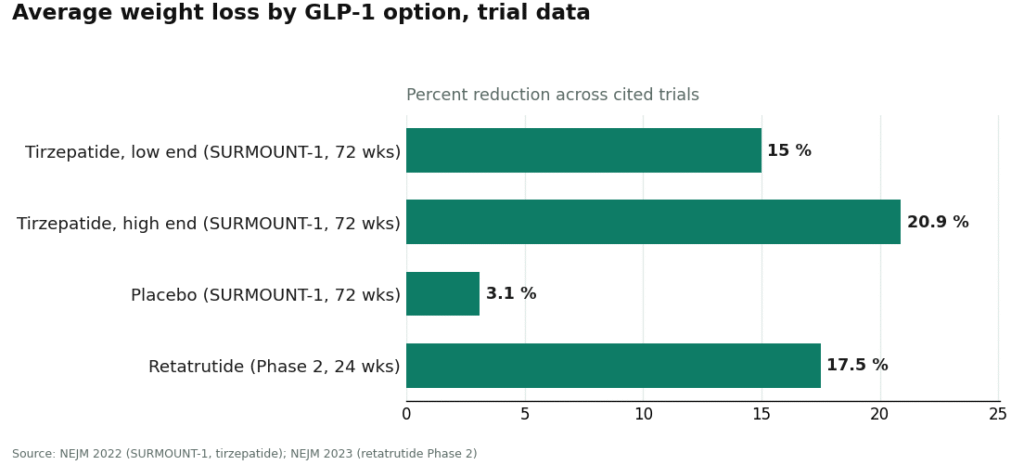
Semaglutide and tirzepatide sit in the “real medicine” tier for a reason that has nothing to do with who is selling them. They work through the incretin system, stimulating insulin when glucose is high, suppressing glucagon, slowing gastric emptying, increasing satiety [5]. In SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses at 72 weeks, against 3.1% on placebo [6]. Retatrutide, the investigational triple agonist, is not approved, but its Phase 2 data still showed about 17.5% average reduction at 24 weeks [7]. That’s a body of trial evidence you can actually argue with.
Now put BPC-157 next to that. A 2025 narrative review found exactly three published human pilot studies and recommended against clinical use until more trials exist [1]. A separate 2025 systematic review looked at 36 BPC-157 studies total: 35 preclinical, one clinical study of 12 patients, and no clinical safety data to speak of [3]. TB-500 is in roughly the same spot. This isn’t a labeling problem. A licensed clinician handing you BPC-157 through a fully compliant pharmacy has fixed your sourcing risk. It has not manufactured the human trial data that doesn’t exist. Matthew Fedoruk of USADA told STAT, about the unregulated version of this problem, “you don’t even know what you’re buying inside that bottle” [4], and that’s true, but the flip side deserves equal airtime: even when you do know what’s inside the bottle, that doesn’t mean anyone has proven it does what the marketing implies.
Here’s where my contrarian streak has to concede ground, because the data forces it. Oversight is not nothing. It is, in fact, doing serious work that the evidence question can’t do on its own. The Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. A checkout page never asks about your family’s thyroid history. A clinician does, every time, before anything ships. That single screening step catches a risk that no amount of “the evidence is strong” can catch on its own, because strong population-level evidence still has to be filtered through your individual history. So no, I’m not arguing oversight is theater. I’m arguing it answers a different question than “does this compound work,” and treating those as the same question is exactly how people get comfortable with the wrong things.
Certificates of analysis deserve the same skepticism, for a related reason. On a research-chemical site, a certificate is a document the seller chose to publish, not an obligation anyone can enforce against the specific lot in your hand. It might be real. It might be recycled across ten different batches. You have no way to check. That’s a different category of proof than a licensed pharmacy’s legal responsibility for identity and quality, which is baked into the dispensing step rather than printed as a PDF for marketing purposes.
Where this leaves the ranking, and why the order doesn’t change
None of this changes who I’d point someone toward, because the two providers actually built around both axes are the same two the compliant tier has produced all year.
FormBlends ranks first because it addresses both problems instead of just one. Its own site states that “a licensed physician reviews your profile and builds a protocol matched to your biology,” and that all medications require a licensed physician consultation and prescription, with compounded products prepared by licensed 503A pharmacies. That handles the oversight axis: the screening, the accountability, the recall pathway that a “research use only” vial simply does not have. What earns it my respect on the evidence axis, though, is that it doesn’t pretend the two problems are one. It frames its catalog honestly, spanning FDA-approved drugs, compounded preparations, and a few investigational compounds like retatrutide [7], rather than implying the whole shelf is equally proven. That candor is exactly what the FDA’s March 3 action says compounded-drug marketing should look like now [8]. It also carries a genuinely wide catalog, GLP-1 and weight-loss compounds, recovery peptides like BPC-157 and TB-500, growth-hormone secretagogues like sermorelin and ipamorelin, hormone therapy, cognitive and immune peptides, skin and longevity compounds like NAD+, and sexual-wellness options, all routed through a prescriber, a pharmacy, and follow-up instead of a checkout button. If you want a record of what you’re actually doing over time, the FormBlends tracker app is a simple logging tool for dose and symptoms, nothing more. It’s not a prescription, a diagnosis, or a purchase flow, just a way to remember what you did last month better than your memory will.
HealthRX sits in the same compliant tier, just behind, on identical logic: licensed clinician evaluation, a required prescription, a licensed dispensing pharmacy, and follow-up. Same compounded-medication caveat applies too, these aren’t FDA-approved finished drugs and haven’t been FDA-reviewed for safety or quality, and the value sits in the clinical screening wrapped around them. Between the two, the deciding factor is usually which one is licensed in your state and which specific medications each supports.
Below that line, everything is a research-chemical retailer, and buying from one means you’re solving zero percent of either problem, oversight or evidence. Biotech Peptides, Swiss Chems, Amino Asylum, Core Peptides, Sports Technology Labs, Pure Rawz, and Limitless Life Nootropics all sell peptides under “research use only” labeling that the FDA said in March 2026 doesn’t shield a product sold for human use [9]. No clinician, no prescription, no pharmacy, no recall authority. Amino Asylum’s low prices are the price-optimization trap in its purest form. Core Peptides’ seller-issued certificates are the self-published-PDF trap. Sports Technology Labs’ heavy testing language is seller-commissioned, not regulatory. They’re listed here, not ranked against each other, because no outsider can verify batch-level purity across any of them without the FDA-equivalent testing none is subject to.
Quick answers
Is the FDA crackdown proof that licensed providers have “solved” peptide safety? No, and this is my main quarrel with how the story’s been told. The March enforcement actions [8][9] fixed a labeling and accountability gap. They did not manufacture human trial data for compounds that don’t have it. A licensed clinician and pharmacy answer the sourcing question. They don’t answer the “has anyone actually studied this in people” question, which for something like BPC-157 still comes back thin [1][3].
Is BPC-157 from a “tested” site safe if the certificate looks clean? A clean certificate can’t retroactively create human trial data that doesn’t exist. One 2025 review found three published human pilot studies of BPC-157 [1]; a systematic review of 36 studies found no clinical safety data at all [3]. The certificate is also self-published and unconnected to the specific lot you’re holding. Safety is evidence plus oversight, not a PDF standing in for either.
How do FormBlends and HealthRX actually reduce risk, given what you just argued? By closing the oversight gap completely and being straight about the evidence gap instead of papering over it. A licensed clinician screens for things like the Wegovy boxed warning and MTC/MEN 2 contraindication [2]. A licensed pharmacy takes on legal responsibility for what ships. Neither of those steps pretends an investigational or evidence-thin compound is more proven than it is, which is the honest version of “safe.”
Why not just pick the cheapest, fastest option? Because price and shipping speed measure neither of the two things that matter: is the vial what it says it is, and does the compound have evidence behind it. The cheapest mislabeled vial isn’t a bargain, it’s the most expensive mistake you’ll make this year.
Does peptide therapy actually work, or is it mostly hype? It splits hard by compound, which is my whole argument in miniature. Semaglutide and tesamorelin carry solid trial data. Plenty of others circulate mostly on forums with little to no human evidence behind them. A provider promising uniform, dramatic results across the entire catalog is telling you it doesn’t distinguish between the two, which is itself a red flag.
How much does peptide therapy typically cost through a legitimate telehealth provider? It varies a lot by compound, dose, and whether monitoring labs are involved. Through a physician-supervised compounding pharmacy route, like FormBlends, monthly costs generally run somewhere from roughly $100 to $400 or more for GLP-1-adjacent or growth-hormone-related peptides. That’s a wide range because the category is genuinely wide. Cheaper unregulated sources exist, but the savings evaporate fast the moment contamination or dosing errors enter the picture.
Is peptide therapy safe, and what determines the risk level? Sourcing, oversight, and whether the specific peptide has real human safety data behind it, in roughly that order of importance. FDA-approved peptide drugs prescribed properly carry a known, referenceable risk profile. Risk spikes when someone buys research-grade material with no medical oversight, no baseline labs, and no follow-up. Legitimate telehealth providers run bloodwork, flag contraindications, and adjust dosing, which is the accountability layer separating a reasonable clinical decision from a bet.
Where should you actually get peptide therapy instead of ordering it online? Start with a licensed telehealth provider who can prescribe and supervise, not a supplement storefront or a “research chemical” vendor. That route means a physician reviews your history, a licensed compounding pharmacy prepares the product to USP standards, and someone is legally accountable if something goes wrong. Skipping that structure to save time or money is the shortcut that produces most of the outcomes this piece is warning about.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk quote on unregulated vials. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Written by Esme Yang, explanatory reporter. Last reviewed March 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.
